
The importance of Infection Controls during the first SARS COVID crisis and readiness it gave for COVID-19
Southeast Asia – 2003
Introduction
During the first coronavirus SARS crisis in 2002/2003, our devices were installed in Hong Kong’s and Singapore’s hospitals, equipping them with the necessary tools to deal with airborne microbe hazards. Infection was quashed and the solutions were a great success.
Today, in this coronavirus SARS2, pandemic, it is evident that these nations are outperforming the world, having as few as 250 recorded COVID19 related deaths intotal since the start of the pandemic back at the end of 2019.
These same germicidal UVC devices were then rolled out around the regions’ key institutional facilities after SARS 2003 across the South East Asia region. China installed UVC in schools, hospitals, critical government buildings and more recently, into their transport network. China’s death toll from this terrible disease is amongst the lowest in the world today, and registers 0 per100,000 of population and yet, one would have expected much worse given the source of the pandemic arose from Wuhan. How?
It is clear, and decades of science and medical evidence from other pathogenic diseases in history says so too – the deployment of germicidal UVC engineered infection interventions in these regions have contributed, along with all the other good practices and measures deployed, to significantly supress COVID-19 cases, mortality, hospitals being overwhelmed, and without the need for the destructive lock-down after lock down alternative interventions resorted to in the “Western world.” For the South East Asian regions, their people have been the safest in the globe and their economies have continued to grow and prosper successfully.
What is SARS?
South Asian Respiratory Syndrome, SARS is a coronavirus that is spread via small aerosol produced by humans a similar way to other Airborne Respiratory Illnesses (ARIs). There is an insignificant transmission rate via surface contact, with most infections being contracted via airborne droplets and aerosol1. SARS-CoV-1, to give it its correct term, mainly affected people between 25 and 70 resulting in a dry cough, breathing difficulties, and an increasing lack of oxygen in the blood, which is the main cause of severe cases and death. SARS was the first pandemic of the 21st century with the virus spreading to 29 countries, including the UK and Canada and infecting at least 8,096 people and reportedly killing 774 2. There were no cases of SARS-CoV-1 reported after 2004.
SARS spread rapidly around the world, largely as a result of infected persons traveling on aircraft to distant cities 3. Due to the airborne nature of the virus, transmission on an aircraft (a confined space) was rapid. In one case a single symptomatic patient caused the infection of 22 other passengers in just 3 hours.
At the start of the SARS outbreak, there was a high quantity of nosocomial (Hospital-acquired) transmission due to lack of non-pharmaceutical interventions to address airborne transmission, “Nosocomial clustering, with transmission to health care workers, patients, and visitors is a prominent feature of the severe acute respiratory syndrome (SARS). Hospital outbreaks of SARS typically occurred within the first week after admission” 4.
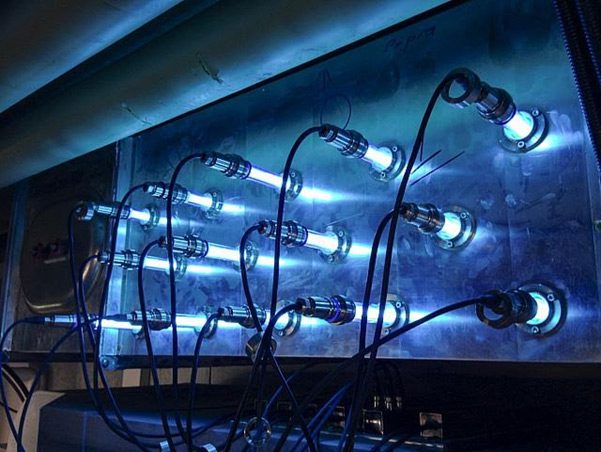
This is what triggered our HVAC germicidal UV devices to be engineered, selected and installed into the duct systems for the total environmental conditions but also infection control locally at the source ie above the patient beds in the wards to intercept and inactivate anything that may have been in the exhaled breath of patients too. A double “global” and “local” infection engineering solution within the buildings.
What is UVC, GUV or UVGI?
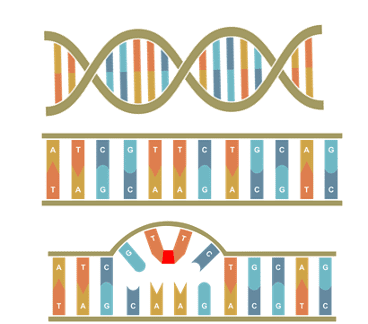
UVC light is also known as germicidal light, or GUV or UVGI. At 254 nm wavelength, UVC renders the DNA and RNA building blocks of microbes inactive by breaking bonds between the Thymine and Adenine proteins, pairing and “glueing” two adjacent Thymine nucleotides together. This process is irreversible with single strand RNA viruses such as coronavirus and stops the microbes from undergoing mitosis, replication or causing harm.
GUV air disinfection has proven efficacy against the transmission of measles, probably one of the most infectious diseases known to mankind, as well as other airborne diseases such as Anthrax, Tuberculosis, SARS-CoV-1, SARS-CoV-2, MERS-CoV, Influenza A, and Avian Influenza, as well as pretty much all other bacteria and viruses known to mankind. These have all been successfully inactivated by GUV Air Treatment solutions in HVAC and via Upper Room Emitters, both in labs, and in practical applications.
SARS-CoV-1, like all other coronaviruses, is easily inactivated by calculated and properly engineered UVC exposure 6 .This data from 2004 shows how easily SARS was inactivated by UV-C technology. It can supress infectious diseases. “The survival ability of SARS coronavirus in human specimens and environments seems to be relatively strong. Ventilation and UV irradiation can efficiently eliminate the viral infectivity”7
What GUV Intervention Measures were Taken and what were the outcomes?
Rapid non-pharmaceutical intervention measures were put into place throughout South East Asia at the start of the first SARS pandemic. This led to our highest quality sterilAir Swiss manufactured products being infection engineered via modelling, deployed and installed in hospitals in Hong Kong and Singapore during that first coronavirus crisis.
In particular, these were extremely effective in high therapy (HDU/ITU) care units within the hospitals. These environments saw significant decreases in the microbial load in the air and successful infection intervention was achieved by the blend of UVC HVAC in-duct and upper room solutions.
Why choose PP-L ?
Our team of chartered engineers, scientists, and medical experts know your environment and your risks, and we help organizations like yourselves go beyond the guidance of governments, to make your inside environments extremely COVID-secure. Our hybrid capability enables us to re-engineer infection and significantly reduce the risk. The technologies and tools that we use to improve COVID security are trusted and reliable solutions that build on decades of scientific data, engineering, practical real-world application and experince. In fact, we are the only government-listed medical services provider of germicidal UV-C health technology in the UK, and we always follow the science.
To see how we can help your workplace, contact us today:
0800 471 4871
Bibliography
(1) World Health Organization. Severe Acute Respiratory Syndrome (SARS) https://www.who.int/health-topics/severe-acute-respiratory-syndrome#tab=tab_1.
(2) CDC. SARS https://www.cdc.gov/sars/about/fs-sars.html.
(3) Olsen, S. J.; Chang, H.-L.; Cheung, T. Y.-Y.; Tang, A. F.-Y.; Fisk, T. L.; Ooi, S. P.-L.; Kuo, H.-W.; Jiang, D. D.-S.; Chen, K.-T.; Lando, J.; Hsu, K.-H.; Chen, T.-J.; Dowell, S. F. Transmission of the Severe Acute Respiratory Syndrome on Aircraft. New England Journal of Medicine 2003, 349 (25), 2416–2422. https://doi.org/10.1056/nejmoa031349.
(4) HO, P.-L.; TANG, X.-P.; SETO, W.-H. SARS: Hospital Infection Control and Admission Strategies. Respirology 2003, 8 (s1), S41–S45. https://doi.org/10.1046/j.1440-1843.2003.00523.x.
(5) Wong, T.; Wallington, T.; McDonald, L. C.; Abbas, Z.; Christian, M.; Low, D. E.; Gravel, D.; Ofner, M.; Mederski, B.; Berger, L.; Hansen, L.; Harrison, C.; King, A.; Yaffe, B.; Tam, T. Late Recognition of SARS in Nosocomial Outbreak, Toronto. Emerging Infectious Diseases 2005, 11 (2), 322–325. https://doi.org/10.3201/eid1102.040607.
(6) Darnell, M. E. R.; Subbarao, K.; Feinstone, S. M.; Taylor, D. R. Inactivation of the Coronavirus That Induces Severe Acute Respiratory Syndrome, SARS-CoV. Journal of Virological Methods 2004, 121 (1), 85–91. https://doi.org/10.1016/j.jviromet.2004.06.006.
(7) Duan, S.-M.; Zhao, X.-S.; Wen, R.-F.; Huang, J.-J.; Pi, G.-H.; Zhang, S.-X.; Han, J.; Bi, S.-L.; Ruan, L.; Dong, X.-P.; SARS Research Team. Stability of SARS Coronavirus in Human Specimens and Environment and Its Sensitivity to Heating and UV Irradiation. Biomedical and environmental sciences: BES 2003, 16 (3), 246–255.
Leave a Reply